Knowledge, Attitude and Practices of Households on Iodized Salt at Urban Slums in Dhaka City
- Mr. Lalit Kumar Sharma; Mr. Sorwar Hossen;
Abstract
Iodine deficiency disorders (IDD) are recognized as a major public health problem in many countries of the world including Bangladesh. Use of iodized salt has been promoted to solve the problem. This study was conducted at 5 urban slums in Dhaka city during May-August 2013 to assess iodine content of salt consumed at household level as well as knowledge, attitude and practice of iodized salt which people of those households possess. A quantitative survey was conducted to collect information and salt samples from 100 households on use of salt. The iodine content of salt sample was determined by laboratory analysis. The results revealed that 88% of the households use iodized salt (iodine content ≥5 ppm) and 82% of the households use adequately iodized salt (iodine content ≥15 ppm). Knowledge about the importance of iodized salt was not adequate. Only, 41% respondents knew one or more benefits of iodized salt. It is encouraging that, 91% of households consume packet salt while 7% of them consume open salt. In addition, 95% of packet salt was iodized; whereas, 22% of open salt was found to be iodized. It is discouraging that IDD Significance of household was mental retardation by 8%, visible goiter by 4%, squint by 3%, deafness by 2%, and dumbness by 2%. Understanding of the coverage and prevalent situation will enable the concerned policy-makers to take pragmatic measures to improve the health condition of people in the urban slum areas by ensuring that all people use adequately iodized salt.
Background of the study
Iodine deficiency disorders (IDD) are recognized as a major global public health problem. According to the latest estimates, about 2.5 billion people worldwide (38% of the world population) have insufficient iodine intake, of which 313 million are in the South – eastern Asian regional (WHO, 2005).
Bangladesh is one of the country in the world which is most affected by iodine deficiency disorders (IDD). The country is the site of the largest river delta in the world. The alleviation of soil by the numerous rivers, together with heavy rainfall and annual flooding, constantly washes iodine from the soil. As such the plant sources are unable to absorb sufficient iodine from the soil. This makes the people of Bangladesh extremely vulnerable to iodine deficiency.
Iodine deficiency is one of the three greatest global public health concerns. It is an essential element required by the thyroid hormone that controls cellular metabolism, neuromuscular tissue growth, and development. A mild iodine deficiency can cause a significant loss of learning ability, as well as other symptoms such as goiter, an abnormal enlargement of the thyroid gland, in its most severe form, iodine deficiency causes cretinism, stillbirth and miscarriage, and increases infant mortality (Delange 1994, 1999). A meta–analysis of 18 studies concluded that iodine deficiency alone lowered mean IQ scores by 13.5 points (Bleichrodt and Born, 1994).
Social and economic effects results from iodine deficiency in both human and animal populations. The World Bank calculated that each dollar dedicated to IDD prevention would yield a productivity gain of $28(Levin et al., 1993).
The virtual elimination of IDD will contribute to the achievement of several of the Millennium Development Goals (MDGs) in Bangladesh by increasing learning ability, school performance and income earning potential, and lowering rates of stillbirths, miscarriages, pregnancy complications of extreme poverty and hunger, achievement of universal primary education, reduction in child mortality and improvement in maternal health.
The Government of Bangladesh is officially committed to IDD elimination through national, as well as international, commitments. The Government of Bangladesh passed the Iodine Deficiency Diseases Prevention Act in 1989. This Act proclaims universal iodization of edible salt for human and animal consumption and included prevention, enforcement and education efforts. Bangladesh Small and Cottage Industries Corporation (BSCIC) of the Ministry of Industries have been assigned to implement, execute and coordinate the Control of Iodine Deficiency Disorders (CIDD) Project. A major objective of the project is to achieve at least 90% household coverage with adequately iodized salt (>15 ppm). Since 1989 United Nations Children's Fund (UNICEF), Micronutrient Initiative (MI), and Global Alliance for Improved Nutrition (GAIN) has been providing financial and technical assistance and policy support to address the alleviation of iodine deficiency problems in Bangladesh through CIDD Project.
There is a considerable decrease in iodine deficiency disorders in Bangladesh, as median urinary iodine levels increased from 54 μg/L in 1993, to 126 μg/L in 1999 and 163μg/L in 2005. The total goitre rate among school-aged children declined from 47.10% in 1993 to 17% in 1999 and 6% in 2005 (Salamatullah and Islam, 1993; Yusuf et al., 2005).Household consumption (iodine content ≥5 ppm) of iodized salt increased from 19% in 1993 to 80.3% in 2012. However, only 57.6 % of the iodized salt was adequately iodized (iodine content ≥15 ppm) in 2012 (Ahmed, 2012).
Now, the principal challenge is to ensure the proper iodization of salt with adequate coverage. Life in slums has always been difficult for the impoverished in urban areas with respect to accommodation standards. Slum dwellers constantly tend to go with poor earnings. They have had different types of nutritional deficiencies among which iodine deficiency is the most notorious one that is still a major nutritional problem. Taking this concern into close consideration, this study has been conducted to make an assessment of the iodine content of salt consumed at household level in the slums of Dhaka city.
To assess iodine content of salt at household level in the urban slums.
To obtain relevant information on the knowledge, attitude and practices of households on iodized salt.
Scope of the study
It should be the norm for all to consume salt that is adequately iodized. The rationale should state that children will have the right to attain their genetic potential, and people will always have the right to find adequately iodized salt in appropriate packages at fair prices at their convenient locations. The population at urban slums is so neglected and deprived a section of the society that they are constantly being bereft of various privileges. They live in unhygienic atmosphere and are always vulnerable to various health hazards. Lower socio-economic setup, poor literacy rate, persistent poverty, darkness of ignorance, and a continuous trauma of negligence perpetuate the issues of malnutrition among which iodine deficiency is considered one of the major nutritional problems.
This study will help us to understand the knowledge level, attitude and practices of Iodized salt and IDD status of people dwelling in urban slums. Considering the mentioned issues, effective communication should be implemented as a fine strategy for the people residing in urban slums. By the dint of the assessment of iodized salt coverage at urban slums area, the concerned department of our Government will develop a sound monitoring system to monitor the production of and retailers’ action for iodized salt.
Limitations of the study
As allocated resources, manpower, and amount of time to conduct the study were very limited, the data along with collection of samples required to be confined in only 100 respondents from 5 urban slums in Dhaka City.Assessment of iodized salt coverage for urinary iodine determination is crucial, but thorough study could not be taken.This study does not assess the coverage of iodized salt at retailer and factory level in comparison with household levels of urban slums.Some respondents did not want to or were even unable to provide reliable data.
SMethodology
This research paper starts with selection of topic and proceeds further with the formulation of objective, fulfillment, the selection of processes, and the collection of data needed for process implementation. Finally, it ends with the submission of the research paper.
Survey area and population
The total number of slums in the Dhaka city is about 4,000 (BDNews, 2013). To conduct this study, only 5 slums were considered which are located at Agargaon, Baganbari, Chalantika, TA Block Slum, and Bhasantek slum. The survey was taken to obtain data on the quality of iodized salt regularly consumed by households. Data and salt samples werecollected from households in urban slum areas at random from June 2013 to August 2013.
Sample size and sampling procedure
Convenience sampling procedure was carefully applied to select the households. Among the 5 urban slums, a total of 100 households from five slums each of which hosts 20 households have been selected.
Data collection method
Households that were selected were visited with a view to collecting relevant information by means of Structural household’s questionnaires. The survey approached cooperative and enthusiastic adults. The survey also collected information on the knowledge, conventional attitude and regular practices of iodized salt. The household selected for salt collection were asked to provide some salt they use when cooking. Salt samples containing approximately 15 grams were obtained in air-tight zip lock bag from the 100 selected households. All samples were properly transferred to air-tight zip lock bag and stored further at room temperature in the CIDD salt testing center laboratory, BSCIC, Dhaka until the analysis for iodine was conducted.
Data management and analysis
Data analysis was conducted with SPSS. Salt was considered as iodized if itiodine contained ≥5 ppm and also defined as adequately iodized if it contained ≥15 ppm of iodine. Each of the survey forms were edited and coded with proper manual labour. Compilation and analysis were undertaken item wise which will successfully address the objective of the study. After completing the compilation along data analysis, a draft of this research paper will be submitted for critical comments and reviews from the honorable supervisor.
Results and Discussion
In the study, a total of 5 urban slums (Agargaon, Baganbari, Chalantika, Ta block and Bhasantek) were selected for the survey in Dhaka city. The plan was to survey 20 households from each slum (20*5=100, actually surveyed 100 households) and one salt sample from each household a total 100 salt sample were collected as per the mentioned in the methodology section.
Household characteristics in the study areas
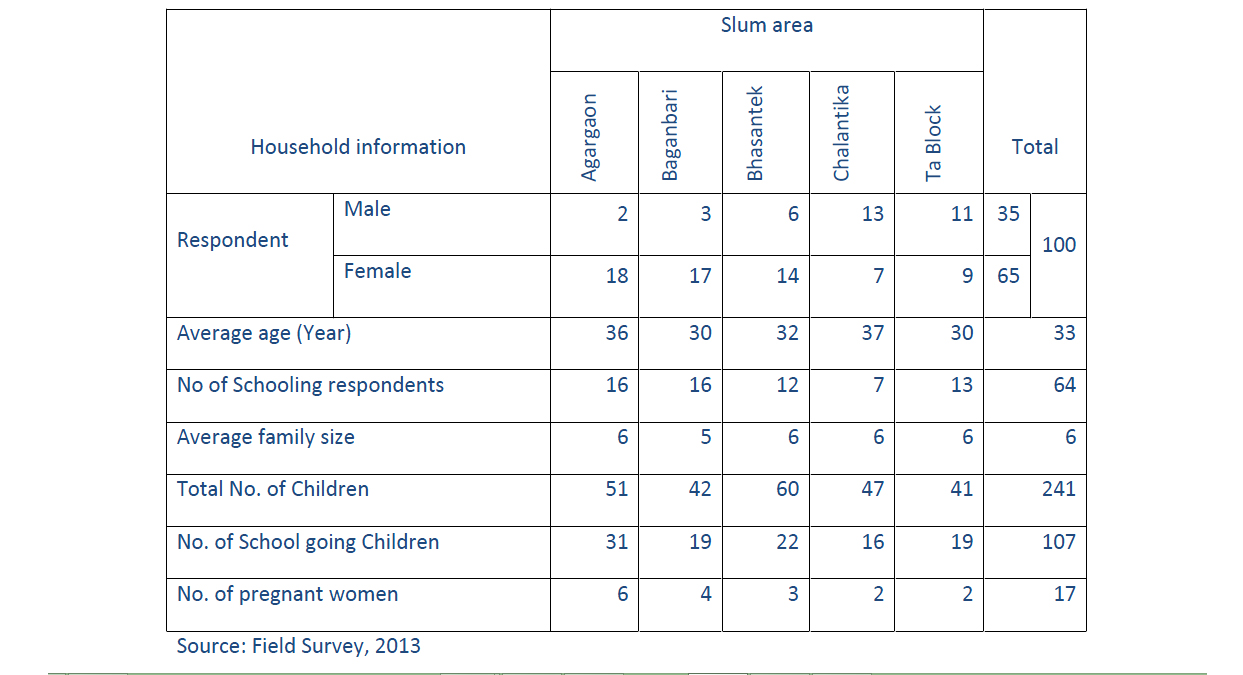
In the household component of the study, table1 show that a total 100 households were surveyed and 35 respondents was male and 65 respondents was female, average age of the respondent was 33 years and 64 respondents were going to school at childhood life. Total household members of the study area were 600 and average family size was 6. Total number of children was 241 whereas 107 children were going to school and pregnant women were 17.
Table1 : Household information of the survey area
Knowledge of household respondents on iodized salt
Figure1 provides information on the knowledge of household respondents of urban slum in Dhaka city on iodized salt. Household respondents informed that they heard about iodized salt (IS) from television, radio, newspaper, health worker, friend or relative, neighbor and other sources. It can be seen from figure 4.1 that in urban slum area 58% household respondents heard about IS from TV, 26% from neighbor, 17% from health worker, 12% from friend or relative and 17 from other sources.
Other factors leading to the trouble
Getting entangled in the sales metrics
The new sales managers or even experienced ones in some occasion seems to get caught in the web of the sales metrics and feeling the pressure from the superior management may in turn persuade him/her in pressurizing his team-members. Here one more commonly observed pitfall is that the subordinate with the highest productivity is pressurized for additional productivity despite his achievement of 100% sales quota to compensate the shortfall contributed by the team members with lower performances rather than trying for improving them. This tactics seems to be workable for a short period as the productive employee under continuous pressure for additional contribution may choose to leave the organization or complain the higher authority on his boss’s behavior.
Figure 1: Source of knowledge on iodized salt in study area
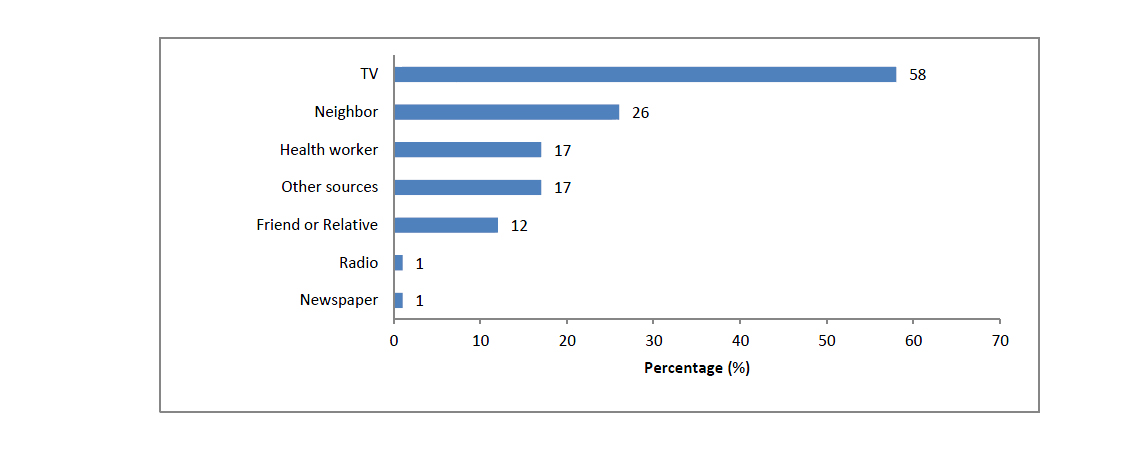
Source: Field Survey, 2013
Figure 2 show that 70% of household respondents had heard about iodized salt and 41% respondents knew one or more benefits of iodized salt, which was considerably lower than the proportion that had heard about iodized salt.
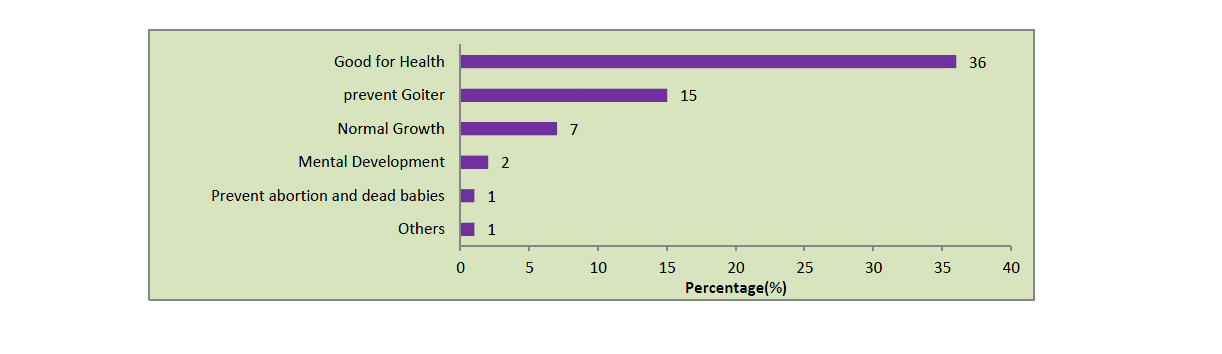
Figure 3 shows that respondents were most familiar with the impact of iodized salt on health which is 36% , 15% answered that intake of iodized salt prevent goiter, 7% told it is need for normal growth, 2% told need for normal development, 1% told prevent abortion and 1% told of others benefit.
Figure 2: Percentage of respondent who had heard of iodized salt and knew at least one benefit of iodized salt
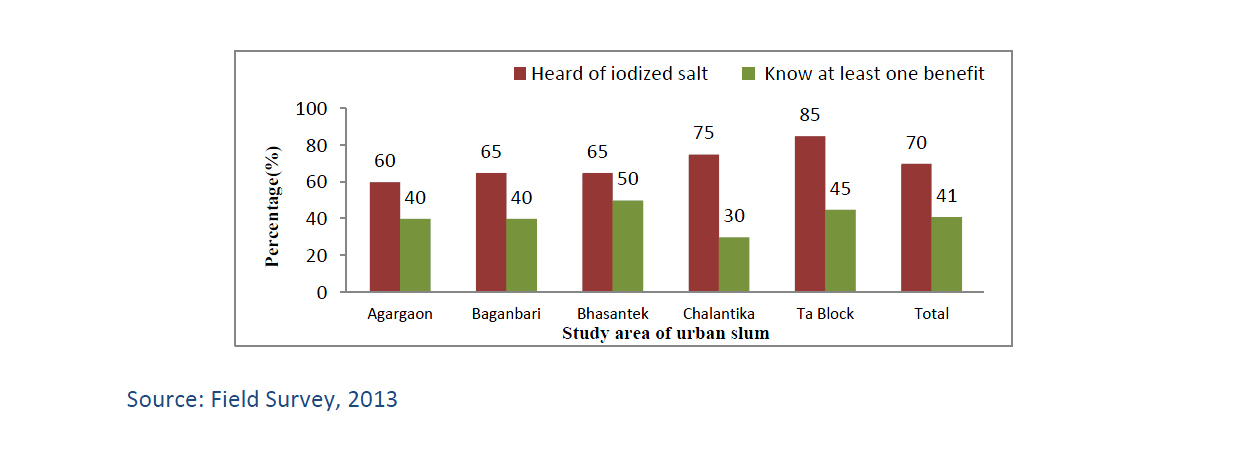
Figure 3: Knowledge of respondent on the benefits of iodized salt
Household practices for purchase, storage and use of salt
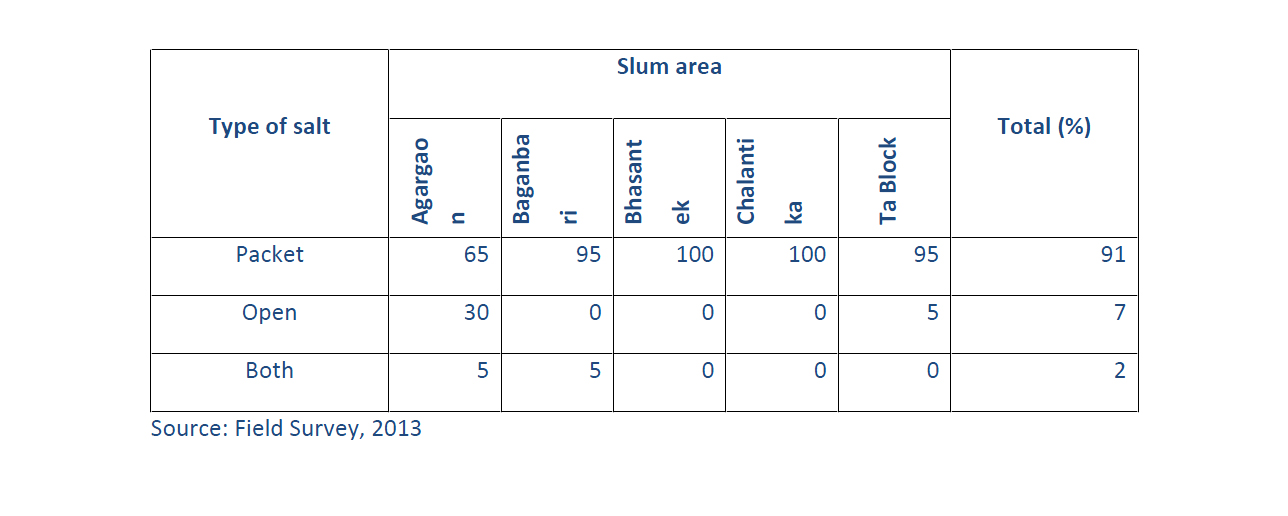
Table 2 show that the most common type of salt consumed by household of urban slums was packet salt (91%), followed by open salt (7%). Only 2% of the household consumed both type of salt.
Table 2: Type of salt used in households (in percentage)
The information of consumption of salt collected from household respondent. Table 3 shows that average of all areas 573 gm. salt consumed per household per week and 13.63 gm. of salt consumed per capita per day. Among the surveyed area household of Bhasantek slum consumed highest level of salt 713 gm. per week and Agargoan slum household consumed low level of salt 518 gm. per week.
Table 3: Salt consumption of urban slums in study area
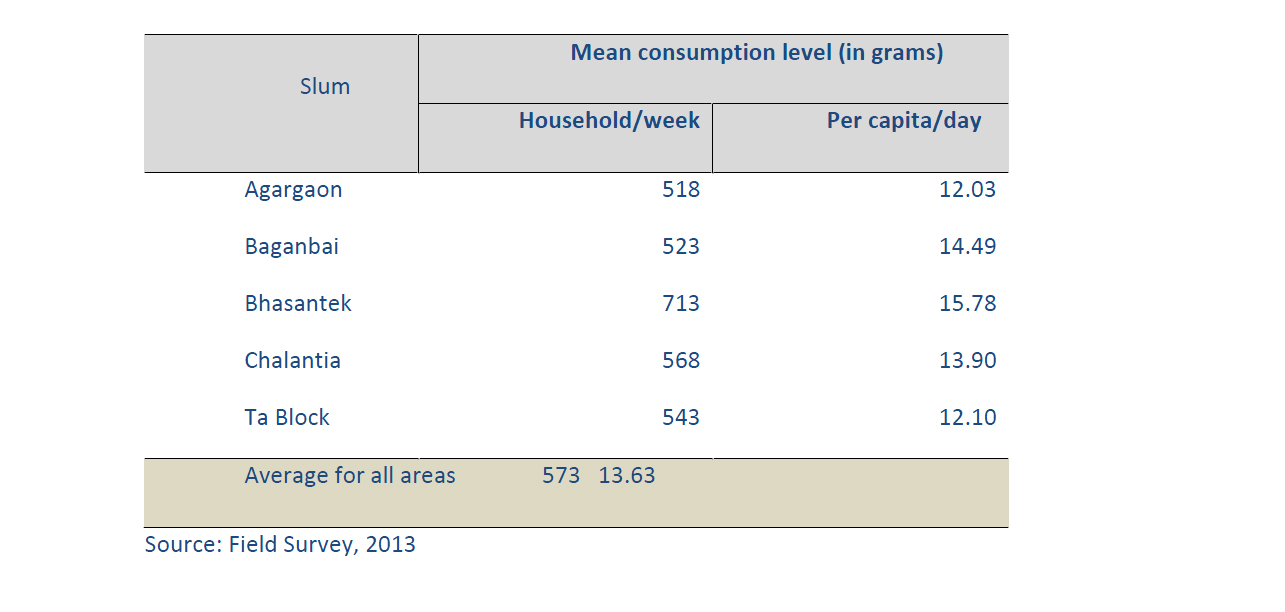
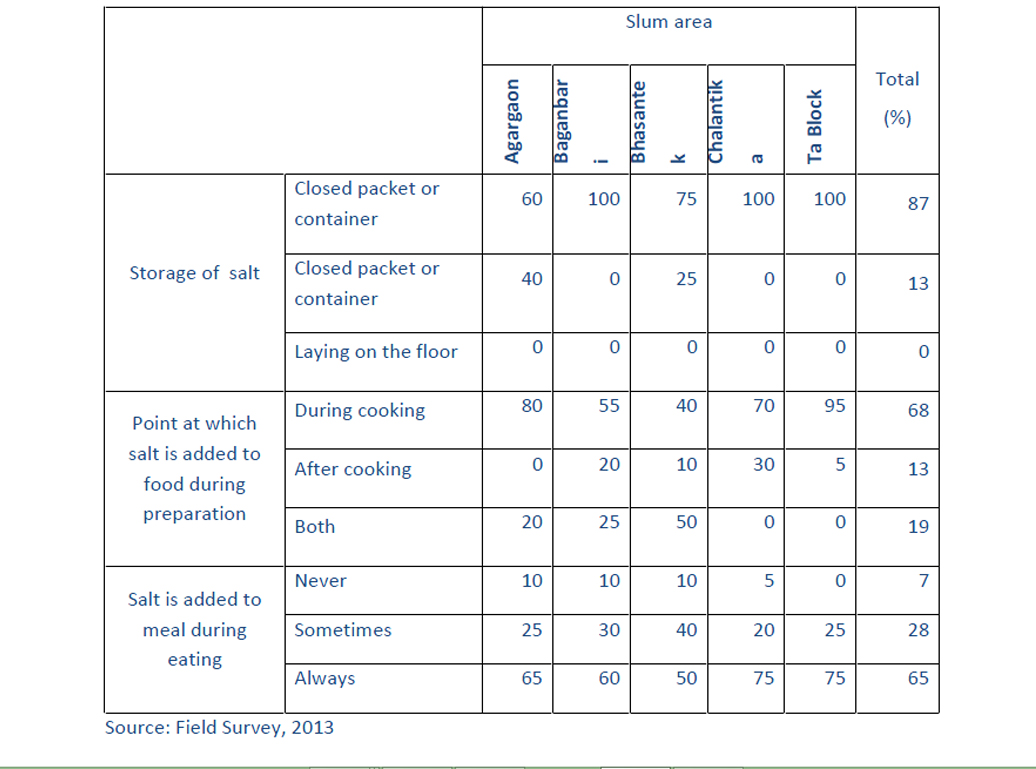
Table 4 shows that most of the households (87%) correctly store salt in a closed packet or container and only 13% household store open packet or container. The majority of household add salt during cooking (68%), only 13% of households add salt after cooking and 19% of households add salt both time of cooking. 65% households always added salt to food during the meal time, 28% sometimes and 7% never.
Table 4: Percentages of household practices for storing and cooking salt
Iodine content of household salt
The iodine content of household salt by the area of urban slums residence is shown in table 5. Totally, 88% sample of household salt was iodized (iodine content 5 ppm), and 82% of household salt was adequately iodized (iodine content 15 ppm). The coverage of iodized salt was considerably highest in Baganbari slum and lowest in Agargoan slum. Banganbari slum coverage of iodized salt 100% and Agargoan slum coverage of iodized salt 65%. Similarly, the coverage of adequately iodized salt was considerably highest in Ta block slum (95%) and lowest in Agargoan slum 60%. Only 7% of household salt was found to contain excessive iodine (50 ppm).
Table 5: Iodine content of household salt in slum area
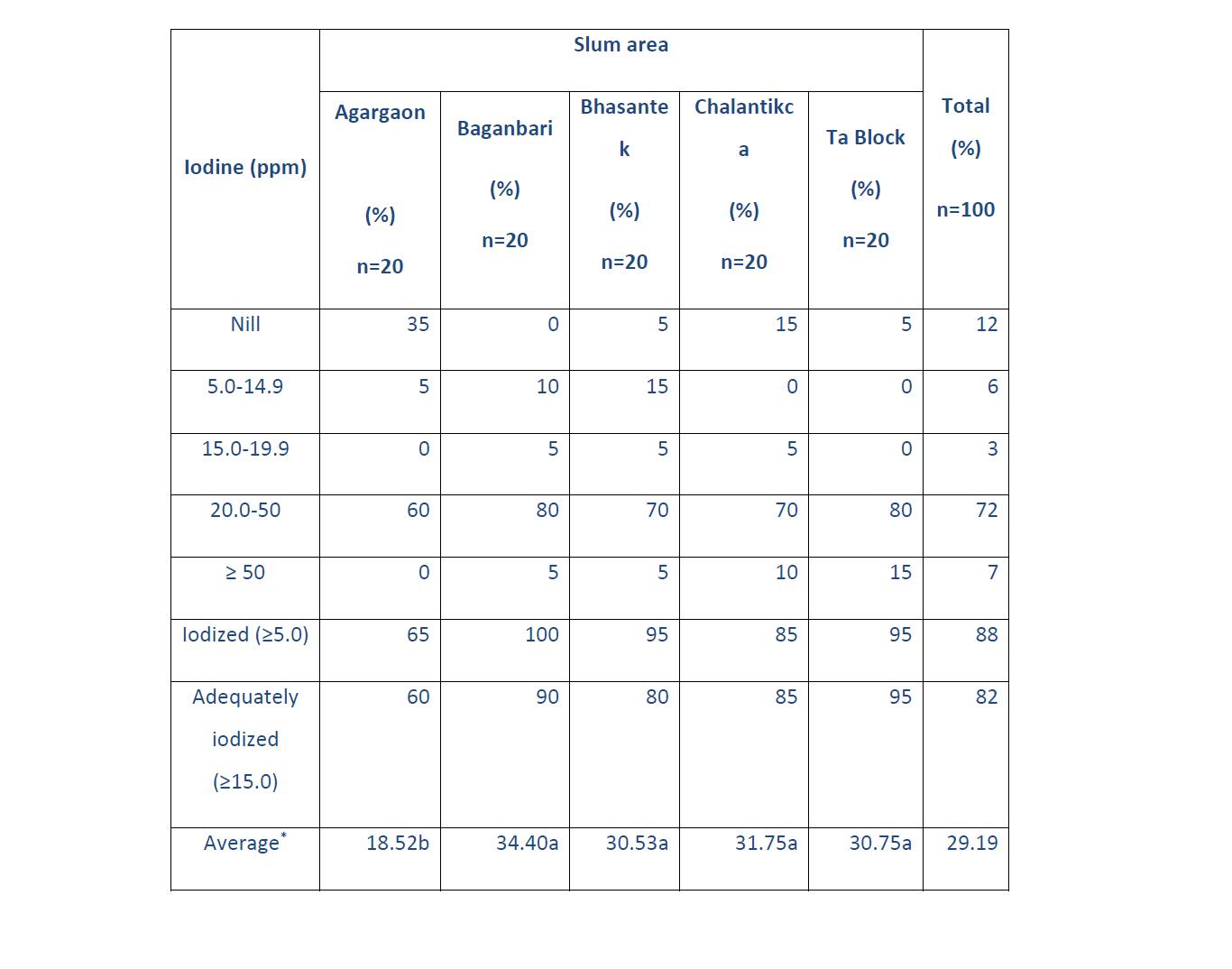
* Same letter indicates insignificant difference and different letter indicates significant difference of iodine content among the slum areas.
Source: Field Survey, 2013
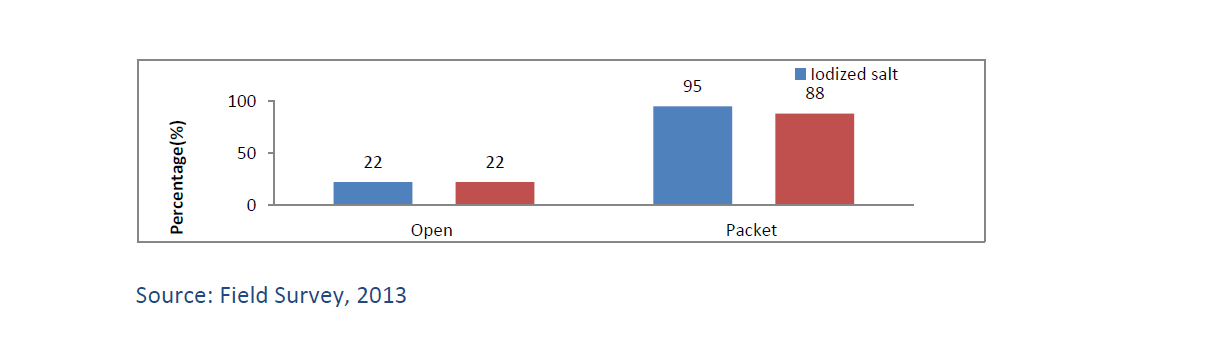
The most common type of salt consumed by the household at urban slum area in Dhaka city was packet salt (91%), followed by open salt (7%) (See table 4.2). Figure 5 show that only 22% of open salt consumed in households was iodized compared with 95% of packet salt, and only 22% of open salt was adequately iodized compared with 88% of packet salt. The quality of open salt is clearly inferior to packet salt.
Figure 5: Percentage of iodized (5 ppm) and adequately iodized (15 ppm) of household salt by the type of salt
Public health significance of IDD in study areas
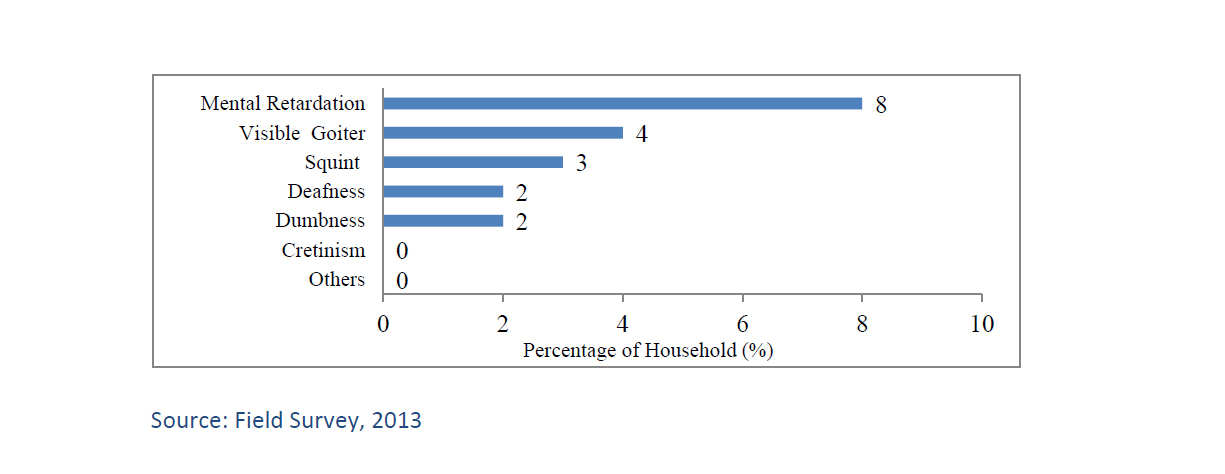
During survey in the urban slum of household physically observe within the household members on IDD Significance and absented of the household members information collected from the household respondent. Result found on IDD significance show in figure 4.6. Highest IDD significance of the household was mental retardation (8%), by the visible goiter (4%), squint (3%), Deafness (2%), Dumbness (2%, cretinism and others (0%).
Figure 6: Percentage of household significance of IDD in urban slum area
Findings and Recommendations
This chapter focused on the overall findings of the study. The study has considered 5 urban slums (Agargaon, Baganbari, Chalantika, Ta block and Bhasantek) in Dhaka city. This study addressed iodine content of salt consumed at household level and knowledge, attitude and practice of iodized salt.
Findings on iodine content of salt consumed at household level
Laboratory analysis of samples found that 88% of household salt samples were iodized (iodine content ≥5 ppm) and 82% were adequately iodized (iodine content ≥15 ppm). The coverage of iodized salt was considerably highest in Baganbari slum and lowest in Agargoan slum. Banganbari slum coverage 100% and agargoan slum coverage 65% of iodized salt. Similarly, the coverage of adequately iodized salt was considerably highest in Ta block slum (95%) and lowest in agargoan slum 60%.
In the study areas average iodine content of the salt samples was 29.19 ppm. Among the slums highest average found in Baganbari slums 34.40 ppm and lowest in Agargoan slum 18.52 ppm. In the study, 22% of households open salt was iodized compared with 95% of packet salt and 22% of households open salt was adequately iodized compared with 88% of packet salt. Only 7% of household salt was found to contain excessive iodine (≥50 ppm).
Findings on knowledge, attitude and practices of households on iodized salt.
Knowledge on the importance of iodized salt was low. In the study, 70% of household respondents had heard of iodized salt and 41% respondents knew one or more benefits of iodized salt..
Household respondents informed that they heard about iodized salt (IS) from television, radio, newspaper, health worker, friend or relative, neighbor and other sources. It can be seen that in urban slum areas 58% household respondents heard about IS from TV, 26% from neighbor, 17% from health worker, 12% from friend or relative and 17 from other sources.
Household respondents were most familiar with the impact of iodized salt on health which is 36% , 15% answered that intake of iodized salt prevent goiter, 7% told it is need for normal growth, 2% told need for normal development, 1% told prevent abortion and 1% told of others benefit.
The most common type of salt consumed by household of urban slums was packet salt (91%), followed by open salt (7%). Only 2% of the household consumed both type of salt. The quality of open salt is clearly inferior to packet salt. The place of purchase salt by household found that 58% of households purchase salt from slum shop and 42% of purchase from nearest bazaar shop..
The information of consumption of salt collected from household respondent and found that average of all areas 573 gm. salt consumed per household per week and 13.63 gm. of salt consumed per capita per day. Among the surveyed area household of Bhasantek slum consumed highest level of salt 713 gm. per week and Agargoan slum household consumed low level of salt 518 gm. per week.
Most of the households (87%) correctly store salt in a closed packet or container and only 13% household store open packet or container. The majority of household add salt during cooking (68%), only 13% of households add salt after cooking and 19% of households add salt both time of cooking. 65% households always added salt to food during the meal time, 28% sometimes and 7% never.
Findings on public health significance of IDD
During study in the urban slum of household physically observe within the household members on IDD significance and absented of the household members information collected from the household respondent. Result found on IDD significance of the households was mental retardation (8%), by the visible goiter (4%), squint (3%), Deafness (2%), Dumbness (2%, cretinism and others (0%).
Recommendations
The recommendations made by this study are stated in the following lines:
The government needs to improve and strengthen the salt law enforcement and monitoring system to stopsupply of non-iodized or inadequately iodized salt at the factory, wholesaler and retailer level before they reach the consumer.
The recommendations made by this study are stated in the following lines:
The government should come forward to sponsor programs to raise awareness among the impoverished section of the country about utility of using iodized salt to improve their mental development and intelligence, potential issues owing to its deficiency, and the ways to get accustomed to taking iodized salt.
Assistance from government sector should be provided to conduct a campaign for consumer and retailer in general to conduct the iodization test of salt using home-based method with rapid testing kits. In addition, prices to buy iodized salt should be kept at a reasonable level so that anyone with any ability can purchase it.
It is imperative to launch an advocacy and communication campaign to garner strong support by all stakeholders for universal salt iodization among the salt industry and retailers and to motivate consumers to use only iodized salt.
Special attention on communication should be given to geographic areas of the country where the coverage of iodized and adequately iodized salt is at low ebb.
Conducting a National IDD and USI Survey in recent times is really helpful enough to measure progress towards universal salt iodization and the elimination of disorders caused by iodine deficiency.
It is also essential to organize advocacy and motivational program for civil society, teachers, social workers, local leader, health worker and religious leaders to disseminate the information on IDD.
Conclusion
In fine, the study aims at addressing the necessity of assessing iodine content of salt at household level at the urban slums in Dhaka city and the country as well. So, awareness and motivation should be the key elements which must be put in place to make people all over the country use properly iodized salt at all levels.
In the study, 88% of household salt samples were iodized (iodine content ≥5 ppm), and 82% were adequately iodized (iodine content ≥15 ppm)..
Knowledge about the importance of using iodized salt was also pretty poor. In the study, 70% of household respondents had ever heard of iodized salt while 41% respondents knew one or more benefits of using iodized salt. However, fewer household respondents made the general statement that using iodized salt is ‘‘good for health” (36%).
It is really inspiring that the most common type of salt consumed by the household in urban slum area was found to be packet salt (91%), followed by open salt (7%).Salt from 22% of households open salt was iodized in comparison with 95% of packet salt.
During the study, physical observation of IDD Significance was found to be the at its highest state by mental retardation which covers 8%, by the visible goiter which covers 4%, squint which covers 3%, deafness which covers 2%, dumbness which covers 2%.
In view of all these findings, we should emphasize the needs to implement some of the mentioned steps on priority basis. The more we can accomplish those pragmatic steps, the more we can hope to get from our salt iodization program.
References
Ahmed, T. (2012). ‘National Micronutrient Status Survey’, October 2012, ICDDRB/UNICEF/GAIN/IPHN, Dhaka, Bangladesh. Bdnews. (2013). 3.5 mn people live in Dhaka slums, Daily Online News, 24 February, p.2. Bleichodt, N. and Born, M.P. (2004). ‘A meta-analysis of research on iodine and its relationship to cognitive development’, New York, USA.
Delange, F. (1994). The disorders induced by iodine deficiency, Postgraduate Medicine Journal, 77(906), 217-220.
DW (2002). ‘An Assessment on the Uprooted Slum Dwellers of Dhaka City’, DemocracyWatch, Dhaka, Bangladesh.
Gulzar, N. (2000). Present Status of Iodized Salt and KAP on Iodized Salt in Different Locations of Dhaka District, Unpublished MS Dissertation, Institute of Nutrition and Food Science, Dhaka University, Dhaka, Bangladesh.
Hetzel, B.S. (1989). ‘The Story of Iodine Deficiency: an International Challenge in Nutrition’, Oxford University Press, New Delhi, India.
HHetzel, B.S. and Pandav, C.S. (1994). ‘S.O.S for a Billion: the Conquest of Iodine Deficiency Disorders’, Oxford University Press, New Delhi, India.
Hetzel, B.S. (1999). Progressive Towards Elimination of Iodine Deficiency Disorders, ICCIDD, New Delhi, India.
Hussein, I. (2011). ‘Strengthening Ties BetweenICCIDDD and the United Arab Emirates, ICCIDD, New Delhi, India.
Levin, H.M., Pollitt, E., Galloway, R. and McGuire, J. (1993). ‘Enriching Lives. Overcoming Vitamin and Mineral Malnutrition in Developing Countries’, World Bank: Washington DC..
Mannar, M.G.V. and Moore, R. (2012). ‘20 Years of Progress’, Micronutrient Initiative, Ottawa, Canada.
Mannar, M.G.V. (2007). ‘Editorial Statement on Eliminating Iodine Deficiency: Learning from an Untold Public Health Success Story’, United Nations System Standing Committee on Nutrition, Lavenham Press, United Kingdom..
Pandav, C.S. and Rao, A.R. (1997). ‘IDD in Livestock: Ecology and Economics’, Oxford University Press, New Delhi, India.
Perez-Lopez, F.R. (2007). ‘Iodine and Thyroid Hormones During Pregnancy and Postpartum’, Gynecological Endocrinology, 23(7), 414-428.
Salamatullah, Q. and Yusuf, H.K.M. (1999). ‘National Iodine Deficiency Disorders Survey’, Dhaka University/IPHN/BSCIC/ICCIDD/UNICEF, Dhaka, Bangladesh.
Salamatullah, Q. and Islam, M.N. (1993). ‘National Iodine Deficiency Disorders Survey1993’, Dhaka University /ICCIDD/ UNICEF, Dhaka, Bangladesh.
Pandav, C.S. and Yadav, K. (2012). ‘Global Iodine Deficiency Disorders Prevention Day Observation across India, ICCIDD, New Delhi, India.
Smyth, P.P. (2006). ‘Dietary iodine intake in pregnancy’, Irish Medical Journal, 99(4), 103-110.
Taylor, S. and Bogdan, R. (1998). Introduction to Qualitative Research Methods: A Guide and a Resource, John Willies and Sons, New York, USA.
WHO (2005). ‘Iodine status worldwide’, WHO Global Database on Iodine Deficiency. World Health Organization(WHO), Geneva.
Yusuf, H.K.M., Khatun, U.H.F. and Rahman, A.K.M. (2005). ‘National Survey on Iodine Deficiency Disorders and Universal Salt Iodization’, Dhaka University /IPHN/BSCIC/ICCIDD/ UNICEF, Dhaka, Bangladesh.
Yadav, K., Pandav, C.S. and Karmarkar, M.G. (2011). ‘Iodized Salt Spreads Across India’, ICCIDD, New Delhi, India.
UNICEF (2004). United Nations Children’s Fund, New York, [online]Available at http://www.kintera.org/site/apps/nlnet/content2. (Accessed on 27 April 2013).
